
Megaloblastic anemia (MBA) may cause a problem in differential diagnosis from other conditions which may cause macrocytosis. Macrocytosis is a normal finding in newborns and during pregnancy but also occurs in alcoholism, hepatic disease, hemolytic states and hypothyroidism. This topic will discuss about laboratory investigations for the differential diagnosis of MBA from those conditions, along with some preliminary investigations.
Hematological Tests
1. Hemoglobin and Hematocrit
According to WHO, the criteria for anemia is when adult males have Hemoglobin levels <13 g/dL and adult females have <12 g/dL. As the iron deficiency worsens, both Hb and PCV decline together.
- Hb >12 g/dl : Not anemic
- Hb 10–11 g/dl : Mild anemia
- Hb 8–9 g/dl : Moderate anemia
- Hb 6–7 g/dl : Marked anemia
- Hb 4–5 g/dl : Severe anemia
- Hb < 4 g/dl : Critical
2. Red Cell Indices
MCV and MCH are increased. MCHC remains normal and RDW is elevated.
- Mean Corpuscular Volume (MCV): It is the average volume of the RBC expressed in femtoliters. It becomes >97 fL in MBA (normal 82–98 fL). MCV values above 125 fl are almost always associated with MBA.
- Mean Corpuscular Hemoglobin (MCH): MCH indicates the amount of Hemoglobin (weight) per RBC and is expressed as picograms. MCH will be >32 pg in MBA (normal 27–32 pg).
- Mean Corpuscular Hemoglobin Concentratration (MCHC): The MCHC measures the average concentration of hemoglobin in a red blood cell. MCHC remains normal in between 31–36 g/dL.
- Red Cell Distribution Width (RDW): RDW is a quantitative measure of anisocytosis. In MBA, RDW is elevated in roughly two-thirds of all cases (normal 11.5–14.5%).
CBC & Peripheral Blood Smear
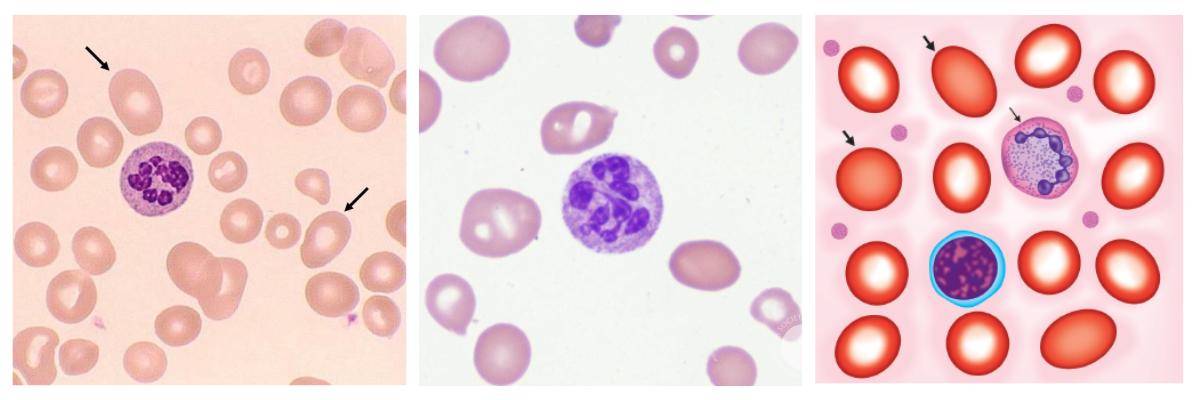
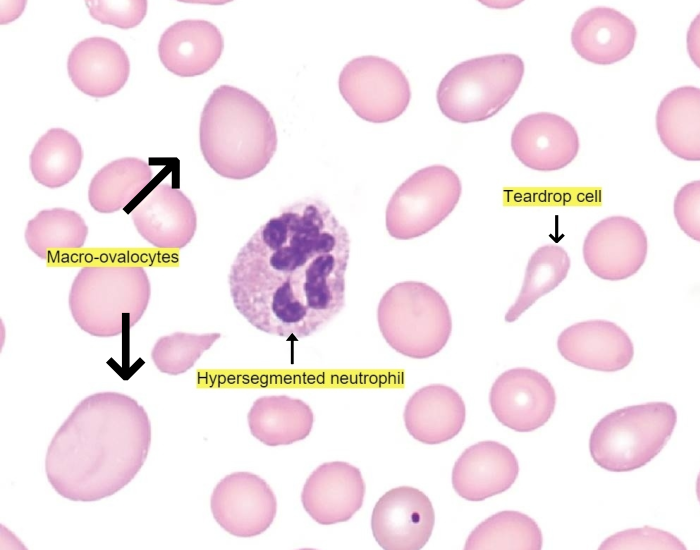
There may be a pancytopenia (decreased RBC, WBC and platelets count). Oval macrocytes, hypersegmanted neutrophils and Howell-jolly bodies are the characteristic triad of abnormalities in megaloblastic anemia.
1. Red Blood Cells (RBCs)
- Macrocytosis: RBCs are usually larger than normal. Macrocytic and oval (egg shaped macro-ovalocyte) is diagnostic feature.
- Most macrocytes lack the central pallor.
- Anisopoikilocytosis: Marked variation in shape and size of the red cells. Ovalocytes, tear-drop cells and some fragmaneted cells are usually found.
- Inclusions: Howell-jolly bodies, Cabot rings and basophilic stippling may be seen.
2. White Blood Cells (WBCs)
- Leukopenia: decreased WBC count.
- Hypersegmented neutrophils (Right shift): When there are at least 5 five-lobed neutrophils per 100 WBCs or at least 1 six-lobed neutrophil is noted.
3. Platelets
Platelet count is usually reduced. Giant platelets may also be observed.
4. Reticulocyte Count
The reticulocyte count is normal or low.
Bone Marrow Examination
- Cellularity: Moderately to markedly hypercellular.
- M:E ratio: Due to marked erythroid hyperplasia, M:E ratio is reversed ranging from 1:1 to 1:6 (normal 2:1 to 4:1).
- Erythropoiesis: Megaloblastic type. Megaloblasts are large, abnormal counterparts of normoblasts showing asynchrony of nuclear and cytoplasmic maturation. As developing megaloblasts die in marrow (intramedullary hemolysis), there is ineffective erythropoiesis.
- Myelopoiesis: Adequate in smaer. May display giant metamyelocytes and band forms.
- Megakaryopoiesis: Normal or increased in number.
- Bone marrow iron: Markedly increased, demonstrated by negative Prussian blue reaction.
Biochemical Tests
| Common Biochemical Tests for both vitamin B12 and Folic acid deficiency | |
|---|---|
| Serum homocysteine | ↑ |
| Serum bilirubin | ↑ |
| Serum iron and ferritin | ↑ |
| Plasma lactate dehydrogenase (LDH) | ↑ |
| Serum vitamin B12/folate | ↓ |
| Specific tests for vitamin B12 deficiency | |
|---|---|
| Serum vitamin B12 levels | ↓ |
Vitamin B12 metabolites:
|
↑ |
| Schilling test | for vitamin B12 absorption |
| Specific tests for Folic acid deficiency | |
|---|---|
| Serum folic acid levels: | ↓ |
| FIGLU in urine | excessively excreted |
very educative